Cluster member Sarah McKetta, working with Lisa Bates, Mark Hatzenbuehler, Bruce Link, Charissa Pratt, and Katherine Keyes, recently published research regarding state-level racism, residential mobility, and Black-White health disparities.
Studies consistently demonstrate that among racial minorities, living in a more racist place is associated with higher levels of illness than living in a less racist place. There are competing theories for why that is the case. One theory is called “social causation,” and posits that racism itself is toxic to health, so living in a racist environment creates poor health directly. A competing theory is called “social selection,” and posits that people who are in better health will move away from more racist environments, effectively leaving behind people who may be sicker or more prone to illness.

State-level racism measured using number of racially-charged Google search terms. Red = highest quartile (most racist); orange = middle-high quartile; yellow = middle-low quartile; green = lowest quartile (least racist)
Using the Panel Study on Income Dynamics, a nationally representative, longitudinal survey of households in the United States, this study attempted to understand the relative contribution of selection vs. causation in determining Black-White health disparities in relation to area-level racism, looking specifically at self-rated health as the outcome of interest. Of note, this paper used a relatively novel measure for racism, a state-level aggregation of Google searches for racial slurs (you can read more about the measure here, here, and here). Using this measure, states were divided into four groups, from low to high, based on their levels of racial animus as measured by Google searches.
The authors showed that overall Blacks had about a 50% higher risk of poor self-rated health than Whites, that living in a state with more racism was associated with poorer health among both Blacks and Whites, and that Blacks were more likely to live in states that scored high on this measure of racial animosity. However, it is possible that these associations could be explained by either selection or causation.
To examine the causation theory, they looked to see if, among people who never moved and had baseline good health, living in racist areas was predictive of developing poor health among Blacks but not Whites. This association was not present, in part because so many people moved at least once, so the authors likely had too few study subjects to detect a difference in health. To examine the selection theory, they looked to see if being healthier at baseline predicted moving out of state, and, specifically, if it predicted moving to a less racist state, particularly among Blacks. They found that, among people who move, better health at baseline was associated with moving out of state, and Blacks in good health tended to move to less racist places.
In sum, this paper demonstrated that selection factors rather than causation may be a more important explanation for these Black-White health disparities. However, the authors believe that neither selection nor causation factors sufficiently explained the magnitude of health disparities between Blacks and Whites. Of the people who moved, 80% of them stayed in the same state, and very few people lived in the states with the lowest level of racial animus. So neither selection nor causation factors alone can sufficiently explain the 50% higher risk of poor health among Blacks compared to Whites.
 The Built Environment and Health Research Group (BEH.Columbia.edu) is looking for candidates to fill a post-doctoral fellow position at the Department of Epidemiology at the Columbia University, Mailman School of Public Health.
The Built Environment and Health Research Group (BEH.Columbia.edu) is looking for candidates to fill a post-doctoral fellow position at the Department of Epidemiology at the Columbia University, Mailman School of Public Health. In new work, Rundle and colleagues find that extensive business travel is associated with poorer behavioral and mental health – smoking, sedentary behavior, trouble sleeping, alcohol dependence, depression and anxiety. The paper was recently
In new work, Rundle and colleagues find that extensive business travel is associated with poorer behavioral and mental health – smoking, sedentary behavior, trouble sleeping, alcohol dependence, depression and anxiety. The paper was recently 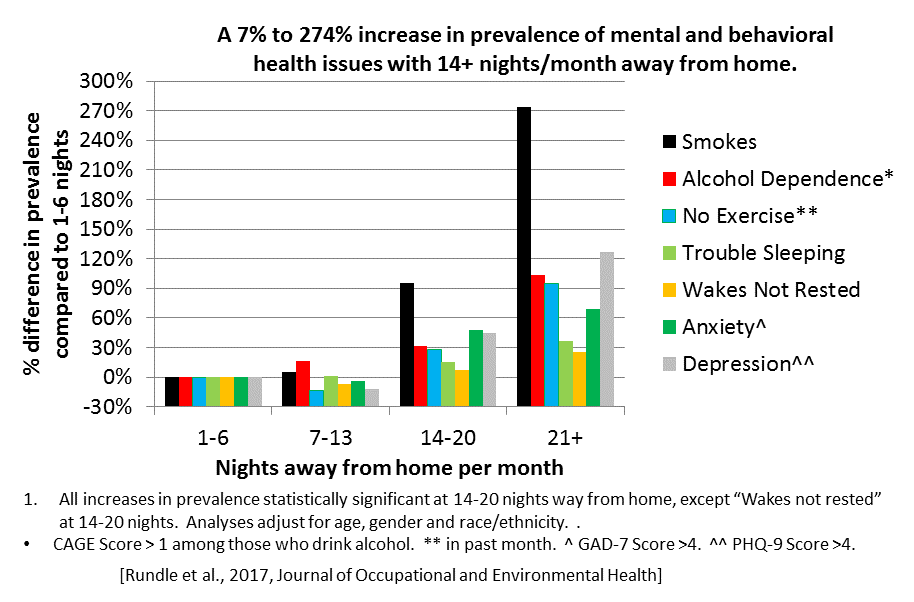
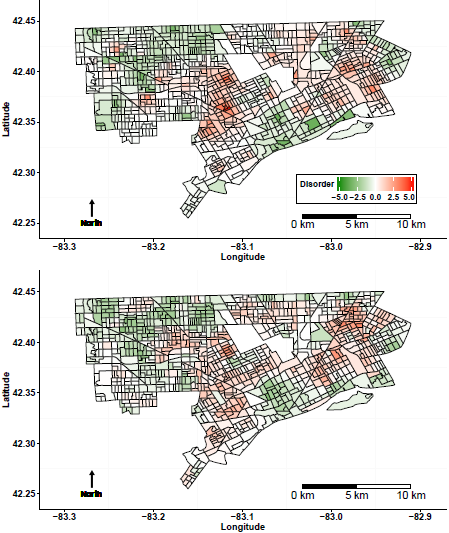 So we took a look at how their measure aligned with ours, and together, we and the DNHS team recently wrote a
So we took a look at how their measure aligned with ours, and together, we and the DNHS team recently wrote a 

 Cluster faculty member, Lisa Bates will receive a 2017 Columbia University Presidential Teaching Award. This award is given to Columbia University’s best teachers for commitment to excellent and often innovative teaching. Bates teaches the Epidemiology Department’s Social Epidemiology Course.
Cluster faculty member, Lisa Bates will receive a 2017 Columbia University Presidential Teaching Award. This award is given to Columbia University’s best teachers for commitment to excellent and often innovative teaching. Bates teaches the Epidemiology Department’s Social Epidemiology Course.