
Depressive symptoms have been spiking among US adolescents for nearly a decade, and the by Noah Kreski and colleagues aimed to examine the role of religious factors in this growing trend.
Historically, religious engagement has been linked to better mental health among adults, typically by fostering hope, coping, and social support. However, studies haven’t examined this dynamic much among adolescents. Religious factors, namely religious service attendance and personal importance of religion, have declined among adolescents since the early 2000’s. If religion is beneficial for them the way it is for adults, this may explain the rise in adolescent depressive symptoms.
Trends in Religious Service Attendance and Personal Importance of Religion and Mean Depressive Symptom Score
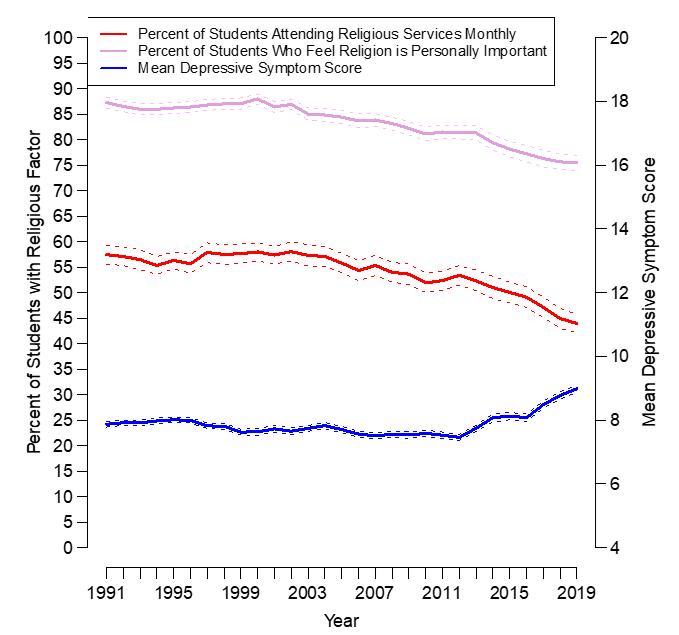
The analysis from Kreski et al. used data from Monitoring the Future, which contains a large, annual, cross-sectional survey of adolescents in grades 8, 10, and 12 (Years: 1991-2019; Total sample size = 417,540). Rather than just examine data on personal importance of religion or religious service attendance separately, they were able to use data from the surveys to identify eight distinct patterns of religious engagement ranging from “feels religion is personally important, attends services weekly” to “feels religion is not personally important, never attends religious services”.
They found that for those who felt religion was personally important, attending services more often was linked to lower depressive symptoms. For adolescents who felt religion was not personally important, the opposite was true; the highest depressive symptoms of any group were found in those who attended services weekly but didn’t feel religion was personally important.
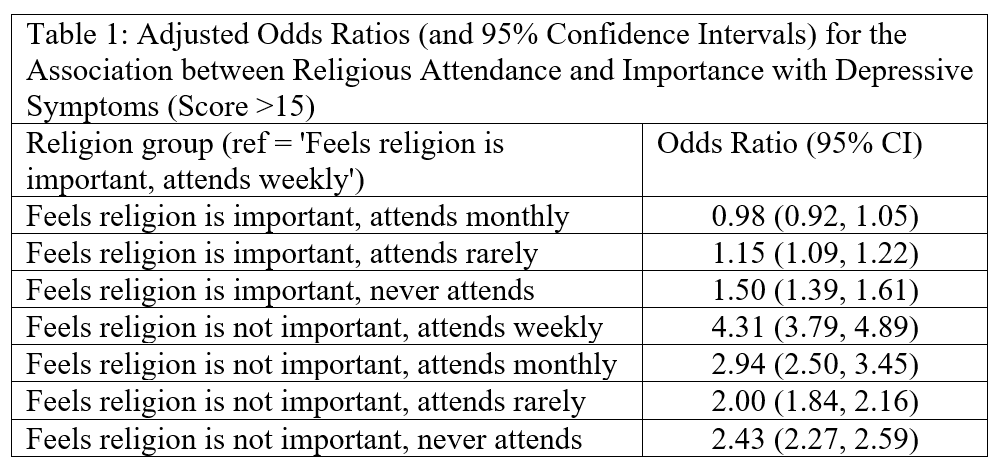
These associations were robust to different cutscores of the outcome scale, and were stronger in the Southern US. While these results help to understand the role of religion in an adolescent’s mental health, the question remains: do shifts in adolescent religious factors explain the recent spike in depressive symptoms?
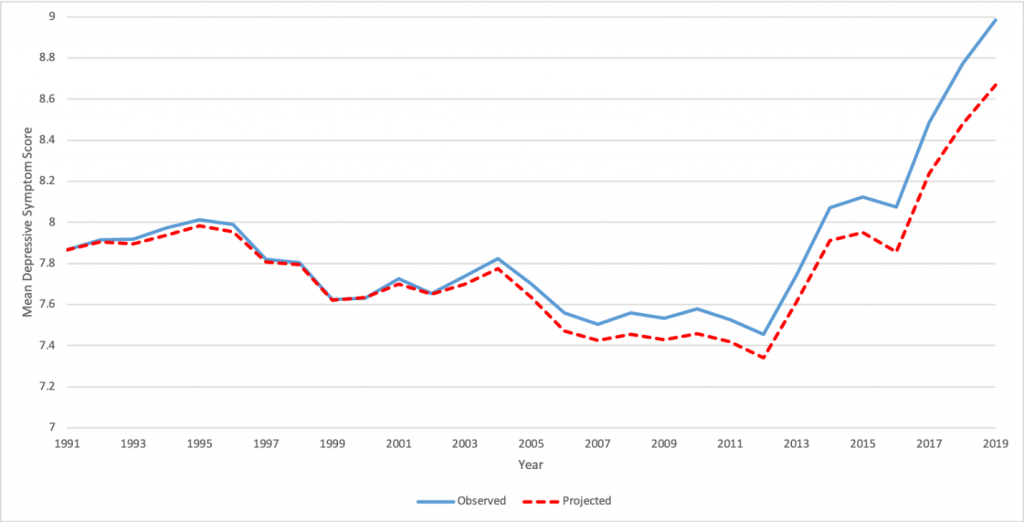
To answer that, Kreski and colleagues needed a different approach, a way to look at what the trend in depressive symptoms would have been if religious factors had stayed static over time. They calculated a projected average depressive symptom score for each year from 1991 to 2019, computed using the year-specific average depressive symptom score for each of the eight religious attendance/importance groups, combined per their 1991 proportions, and compared the projections to the observed data. The observed and projected trends in adolescent depressive symptoms can be seen below:
Observed and Projected Major Depressive Symptom Score
Observed and Projected
The widening gap seen in the graph between the observed and projected trends suggests that over time, a substantial component of the rise in adolescent depressive symptoms could be explained with shifts in religious engagement. Overall, the rise in depressive symptoms from 1991 to 2019 would be 28.2% lower if religious factors had remained at 1991
Religion is a deeply personal experience, and if it’s important to an adolescent, encouraging their attendance of religious services may be a step towards better mental health. If religion isn’t personally important to an adolescent, they shouldn’t be pushed into attending services, but instead receive social support and coping strategies from other sources.