
Estimating Epidemiological Characteristics of SARS-CoV-2 Variants of Concern / Interest
We did a serial of studies on estimating the epidemiological properties of SARS-CoV-2 several variants of concern (VOCs) or variant of interest (VOI); these include 1) development of a model-inference method to estimate the changes in transmissibility and immune escape potential, with applications to the Alpha, Beta, and Gamma VOCs; 2) studying the COVID-19 pandemic dynamics in India, the rise of the Delta VOC therein, and implication to vaccination; 3) characterization of the B.1.526 (i.e. Iota) VOI, including the early dynamics in the NYC neighborhood it was first detected, the changes in transmissibility and immune escape potential, and infection fatality risk; and 4) studying the pandemic dynamics in the nine provinces in South Africa and epidemiological characteristics of the Omicron variant. A brief description to each study below.
Development of a model-inference system for estimating epidemiological characteristics of SARS-CoV-2 variants of concern
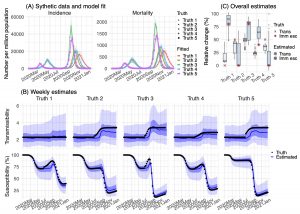 To support COVID-19 pandemic planning, we develop a model-inference system to estimate epidemiological properties of new SARS-CoV-2 variants of concern (VOCs) using case and mortality data while accounting for under-ascertainment, disease seasonality, non-pharmaceutical interventions, and mass-vaccination. Applying this system to study three VOCs, we estimate that B.1.1.7 has a 46.6% (95% CI: 32.3 – 54.6%) transmissibility increase but nominal immune escape from protection induced by prior wild-type infection; B.1.351 has a 32.4% (95% CI: 14.6 – 48.0%) transmissibility increase and 61.3% (95% CI: 42.6 – 85.8%) immune escape; and P.1 has a 43.3% (95% CI: 30.3 – 65.3%) transmissibility increase and 52.5% (95% CI: 0 – 75.8%) immune escape. Model simulations indicate that B.1.351 and P.1 could outcompete B.1.1.7 and lead to increased infections. Our findings highlight the importance of preventing the spread of VOCs, via continued preventive measures, prompt mass-vaccination, continued vaccine efficacy monitoring, and possible updating of vaccine formulations to ensure high efficacy.
To support COVID-19 pandemic planning, we develop a model-inference system to estimate epidemiological properties of new SARS-CoV-2 variants of concern (VOCs) using case and mortality data while accounting for under-ascertainment, disease seasonality, non-pharmaceutical interventions, and mass-vaccination. Applying this system to study three VOCs, we estimate that B.1.1.7 has a 46.6% (95% CI: 32.3 – 54.6%) transmissibility increase but nominal immune escape from protection induced by prior wild-type infection; B.1.351 has a 32.4% (95% CI: 14.6 – 48.0%) transmissibility increase and 61.3% (95% CI: 42.6 – 85.8%) immune escape; and P.1 has a 43.3% (95% CI: 30.3 – 65.3%) transmissibility increase and 52.5% (95% CI: 0 – 75.8%) immune escape. Model simulations indicate that B.1.351 and P.1 could outcompete B.1.1.7 and lead to increased infections. Our findings highlight the importance of preventing the spread of VOCs, via continued preventive measures, prompt mass-vaccination, continued vaccine efficacy monitoring, and possible updating of vaccine formulations to ensure high efficacy.
For details, please see:
Yang, W., Shaman, J. Development of a model-inference system for estimating epidemiological characteristics of SARS-CoV-2 variants of concern. Nat Commun 12, 5573 (2021).
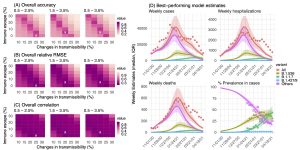
 The Delta (i.e., B.1.617.2) SARS-CoV-2 variant of concern has spread quickly worldwide. Studies have indicated that Delta is able to evade prior immunity and estimated a 60-120% increase in transmissibility, explaining its quick global spread. However, unlike many places seeing a prolonged Delta pandemic wave, the COVID-19 Delta pandemic wave in India surged and declined within 3 months; cases then remained low despite the continued spread of Delta elsewhere. In this study, we utilize comprehensive model-inference methods to estimate key epidemiological characteristics of the Delta variant based on data from India and examine the underpinnings of its dynamics. In addition, we utilize the large discrepancy in one- and two dose vaccination coverage in India (53% vs. 23% by end of Oct 2021) to examine the impact of vaccination and whether prior non-Delta-infection can boost vaccine effectiveness (VE), a phenomenon reported in laboratory studies but has not been examined at the population level.
The Delta (i.e., B.1.617.2) SARS-CoV-2 variant of concern has spread quickly worldwide. Studies have indicated that Delta is able to evade prior immunity and estimated a 60-120% increase in transmissibility, explaining its quick global spread. However, unlike many places seeing a prolonged Delta pandemic wave, the COVID-19 Delta pandemic wave in India surged and declined within 3 months; cases then remained low despite the continued spread of Delta elsewhere. In this study, we utilize comprehensive model-inference methods to estimate key epidemiological characteristics of the Delta variant based on data from India and examine the underpinnings of its dynamics. In addition, we utilize the large discrepancy in one- and two dose vaccination coverage in India (53% vs. 23% by end of Oct 2021) to examine the impact of vaccination and whether prior non-Delta-infection can boost vaccine effectiveness (VE), a phenomenon reported in laboratory studies but has not been examined at the population level.- Using model-inference estimates from March 2020 to June 2021, we estimate Delta escaped immunity in roughly one-third of individuals with prior wildtype infection and was around 60% more infectious than wildtype SARS-CoV-2. Here we have removed the effects of location-specific population susceptibility, intervention measures, and infection seasonality; thus, these results are variant-specific.
- Predicted cases and deaths during July –Oct 2021 were most accurate when models assumed higher VE among those with prior non-Delta infection, particularly after the 1stdose (best-performing VE setting: 90/95% vs. 30/67% baseline for the 1st/2nddose). Counterfactual modeling indicates that high vaccination coverage for 1stvaccine dose in India combined with the boosting of VE among recoverees, averted around 60% of infections during July – Oct 2021. These findings support the effectiveness of 1-dose vaccination for recoverees and suggestprioritizing first-dose vaccination may be an effective strategy for mitigating COVID-19 burden in countries with high underlying SARS-CoV-2 infection rates, given continued vaccine shortages.
- We show that non-pharmaceutical interventions, infection seasonality, and high coverage of 1-dose vaccination likely all contributed to pandemic dynamics in India during 2021.
For details, please see:
COVID-19 pandemic dynamics in India, the SARS-CoV-2 Delta variant, and implications for vaccination
Epidemiological characteristics of the B.1.526 SARS-CoV-2 variant
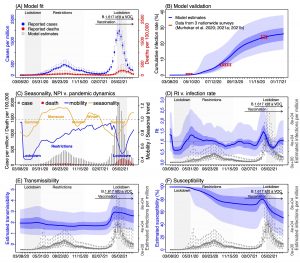
 The B.1.526 variant (WHO designation: Iota), a SARS-CoV-2 Variant of Interest (VOI), was identified during Nov 2020 and quickly became a predominant variant in the New York City (NYC) area. It has also been detected in all 52 states/territories in the US and at least 27 other countries (GISAID data, as of 6/9/2021). An initial laboratory study (Annavajhala, et al. 2021) suggested that this variant is to some extent resistant to two therapeutic monoclonal antibodies in clinical use and neutralization by convalescent plasma and vaccinee sera. However, another study (Thompson et al. 2021) examined all sequenced B.1.526 cases in NYC identified as of April 5, 2021 (n = 3,679) and showed preliminary evidence that this variant did not increase risk for infection after vaccination or reinfection. Given these discrepancies, in this study we utilize detailed population epidemiological data collected since the beginning of the COVID-19 pandemic in NYC (March 1, 2020 – April 30, 2021) and multiple model-inference methods to estimate the transmissibility, immune escape potential, and disease severity of B.1.526.
The B.1.526 variant (WHO designation: Iota), a SARS-CoV-2 Variant of Interest (VOI), was identified during Nov 2020 and quickly became a predominant variant in the New York City (NYC) area. It has also been detected in all 52 states/territories in the US and at least 27 other countries (GISAID data, as of 6/9/2021). An initial laboratory study (Annavajhala, et al. 2021) suggested that this variant is to some extent resistant to two therapeutic monoclonal antibodies in clinical use and neutralization by convalescent plasma and vaccinee sera. However, another study (Thompson et al. 2021) examined all sequenced B.1.526 cases in NYC identified as of April 5, 2021 (n = 3,679) and showed preliminary evidence that this variant did not increase risk for infection after vaccination or reinfection. Given these discrepancies, in this study we utilize detailed population epidemiological data collected since the beginning of the COVID-19 pandemic in NYC (March 1, 2020 – April 30, 2021) and multiple model-inference methods to estimate the transmissibility, immune escape potential, and disease severity of B.1.526.
We estimated that B.1.526 had a moderate increase (15-25%) in transmissibility and could escape immunity in 0-10% of previously infected individuals. In addition, B.1.526 substantially increased the infection-fatality risk (IFR) among adults 65 or older by >60% during Nov 2020 – Apr 2021, compared to baseline risk estimated for preexisting variants. Overall, findings suggest that new variants like B.1.526 likely spread in the population weeks prior to detection and that partial immune escape (e.g., resistance to therapeutic antibodies) could offset prior medical advances and increase IFR. Early preparedness for and close monitoring of SARS-CoV-2 variants, their epidemiological characteristics, and disease severity are thus crucial to COVID-19 response as it remains a global public health threat.
For details, please see:
SARS-CoV-2 transmission dynamics in South Africa and epidemiological characteristics of the Omicron variant
Within days of first detection, Omicron SARS-CoV-2 variant case numbers grew exponentially and spread globally. To better understand variant epidemiological characteristics, we utilize a model-inference system to reconstruct SARS-CoV-2 transmission dynamics in South Africa and decompose novel variant transmissibility and immune erosion. Accounting for under-detection of infection, infection seasonality, nonpharmaceutical interventions, and vaccination, we estimate that the majority of South Africans had been infected by SARS-CoV-2 before the Omicron wave. Based on findings for Gauteng province, Omicron is estimated 100.3% (95% CI: 74.8 – 140.4%) more transmissible than the ancestral SARS-CoV-2 and 36.5% (95% CI: 20.9 – 60.1%) more transmissible than Delta; in addition, Omicron erodes 63.7% (95% CI: 52.9 – 73.9%) of the population immunity, accumulated from prior infections and vaccination, in Gauteng.
For details, please see:
SARS-CoV-2 transmission dynamics in South Africa and epidemiological characteristics of the Omicron variant,