
Creating this post to retain this site and migrated to the new platform.
-
Recent Posts
Recent Comments
Creating this post to retain this site and migrated to the new platform.
The Multistate Pharmacy Jurisprudence Examination (MPJE) is a law exam that pharmacists must pass to practice in most U.S. states. While a few states—such as Idaho and Ohio—do not require the MPJE, and California administers its own version known as the CPJE (which emphasizes clinical aspects of pharmacy practice), the MPJE remains a requirement for licensure in nearly all other states.
Many pharmacy graduates and licensed pharmacists seeking to practice in a different state find the MPJE particularly challenging. Law and regulatory topics are areas most pharmacists are neither deeply trained in nor comfortable with. The purpose of this post is to offer practical tips not only to improve your chances of passing the MPJE but also to help reduce the time, stress, and uncertainty associated with preparing for it.
You might reasonably ask, “Who are you to be giving advice on the MPJE?” It’s a fair question. After all, advice on a specialized pharmacy law exam coming from someone trained in data analytics may seem out of place. However, as of the date of this writing, I have passed ten MPJE exams on my first attempt—eight of them within a two-month span. At one point, I was taking one MPJE per week, with as little as four days between exams, due to the demands of my job, which required multistate licensure.
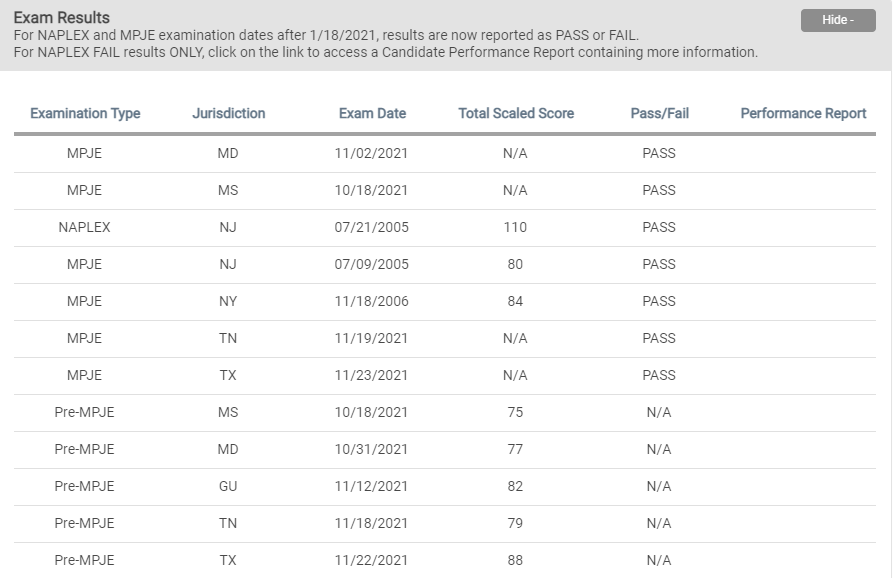
*Note: Guam result is not reported via NABP but I passed.
The above outlines my current progress with MPJEs. I was able to achieve passing scores while working 48 hours per week. Now, I’m not trying to brag about my time management skills or test-taking abilities (well—maybe just a little when it comes to time management), but my main point is this: preparing for the MPJE doesn’t need to take weeks or months of studying.
I’ve seen interns dedicate three months to studying for a single MPJE—longer than many people spend preparing for the bar exam! In my experience, about 20 hours of focused study is more than enough for the first MPJE. For subsequent exams, assuming your knowledge of federal law hasn’t completely faded, 8 hours of review is typically sufficient.
To be fair, the MPJE is a difficult exam. Personally, I found my first MPJEs—New Jersey (07/09/2005) and Mississippi (10/18/2021), which I consider equally “first” due to the 16-year gap—more challenging than the New York State Bar Exam. My pharmacist colleagues often laugh when I say this, but I genuinely mean it.
Why? Because unlike the bar exam, the wording of some MPJE questions is so convoluted that it can confuse even a licensed attorney with over 15 years of pharmacy experience across various settings. At least on the NYS Bar Exam, you can showcase your understanding through essays—demonstrating how laws apply and what outcomes are likely. The MPJE, however, is entirely multiple choice, often with “Select All That Apply” (SATA) questions, offering no opportunity to explain your reasoning.
By the way—don’t panic if you get several SATA questions in a row. That’s actually a good sign! While the NABP doesn’t release details about how the MPJE is scored (other than noting it’s adaptive), I believe SATA questions appear only when you’re performing well. Think about it: if you keep getting answers wrong, the algorithm likely responds with easier questions. To “unlock” those trickier SATA items, you probably need a streak of correct responses. So, if you’re seeing back-to-back-to-back SATA questions, chances are you’re doing great.
Conversely, if you don’t see many SATA questions—or if you get one here and there, followed by something overly simple like “Do you need a license to practice pharmacy?”—that might be a red flag. Again, this is purely my theory based on the adaptive nature of the exam, but I’m fairly confident it holds water.
Even though the MPJE is tough, achieving a passing score of 75 out of 100 shouldn’t be too difficult—if you know what to focus on. Keep in mind, a score of 75 doesn’t mean you need 75% of the questions correct. It’s a scaled score. NABP doesn’t disclose how scaling works, but in my opinion (again, speculative), correctly answering around 50% of the graded questions may be enough to pass. Remember, 20 out of the 120 questions are experimental and don’t count toward your score.
So, what do I study when preparing for the MPJE?
Most of the information can be found using the search function on each state’s pharmacy laws, rules, and regulations page—many states even offer them in downloadable PDFs. I also highly recommend reading the Board of Pharmacy’s FAQ section. These FAQs often clarify topics that are vague or confusing in the statutes, and they directly reflect real-world areas where pharmacists commonly struggle. In fact, I’ve seen questions pulled directly (sometimes verbatim) from state FAQ pages appear on the actual MPJE—making them rare freebies if you’ve read them in advance.
In addition, make sure to review recent Board of Pharmacy newsletters or letters (available via NABP or state board websites). These documents often contain the board’s interpretations of pharmacy laws in areas where compliance issues are frequent. Like the FAQs, I’ve frequently encountered exam questions based on these letters. Believe it or not, they’re often quite interesting—they cover the most debated or relevant topics of the moment.
Below, I’ll share the exact list of legal topics I always study before an MPJE. For clarity, I don’t study anything outside of these topics. If a question appears on something I didn’t cover, I just make an educated guess and move on. Remember: the goal isn’t to ace the exam. The goal is to hit that passing scaled score of 75—which, based on my experience, is achievable even if you have to guess on a handful of questions. And if you’ve studied federal law thoroughly, your “educated guesses” likely have a pretty decent chance of being correct.
Federal law serves as the foundation for every state’s MPJE, as the exam essentially tests three components: federal law, the state’s modifications to federal law, and state-specific laws not addressed by federal statutes. In other words, if the state law is silent on a particular issue, pharmacists must defer to the federal law. It is important to understand that when federal and state laws conflict, pharmacists must follow the stricter of the two. While state laws are often more stringent, there are exceptions – particularly regarding controlled substances – where federal law may be stricter.
Therefore, it is essential to first learn and memorize federal law before reviewing state-specific regulations. Establishing a solid foundation in federal law will make it easier to understand how each states builds upon or deviates from it. .
The list is not comprehensive and make sure you understand what effect the laws and regulations you encounter during your studies have on current pharmacy practice.
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
For example, is NDC number required on the label of the vial dispensed to the patient at a retail pharmacy?
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
How about on the labels of unit-dosed packages in an inpatient setting?
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
Know the eligibility requirements for a facility to register as a 503B outsourcing facility with the FDA.
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
No other healthcare professionals other than pharmacists are required to pass a law exam to practice. Doctors, nurses, dentists, physician assistants, and others only need to demonstrate their clinical knowledge and practical skills prior to licensure. What makes pharmacists different from others? The major difference is that the pharmacists are involved in moving large amounts of controlled substances. Pharmacists must know every aspect of the controlled substance law as pharmacists order, store, distribute, and dispense controlled substances. In addition to the complex regulations on controlled substances, many states relying on pharmacists to identify inappropriate prescribing and dispensing of controlled substances in effort to combat opioid epidemic makes controlled substance law not only a key component, but also the most frequently asked topic in the MPJE.
The most effective way to study controlled substance laws is to categorize them based on real-world scenarios commonly encountered in pharmacy practice.
A good starting point is when pharmacists receive a prescription for a controlled substance.
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
Other common scenarios include ordering, receiving, storing, sending, selling, and dispensing controlled substances.
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
Know the common DEA forms and registration rules: Which form is used to report theft or loss of controlled substance (DEA-106)? Destruction of controlled substances (DEA-41)? Registration (DEA-224)? How long is DEA registration good for? Does hospital pharmacy department with multiple satellite pharmacies require separate DEA registrations?
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
Understanding laws involving non-controlled substances are just as important as the controlled substance laws as most pharmacists will spend majority of their time dispensing non-controlled substances during their practice. The initial approach reviewing non-controlled substance prescriptions is the same as for controlled substance prescriptions.
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
Pharmacists must have a foundational understanding of pharmacy operations on all practice settings, not just hospital or community settings. In particular, you must know what part of operations can be performed only by a licensed pharmacist. Also, know which tasks can be delegated to pharmacy interns, externs, licensed/certified techs, non-licensed/certified techs, and clerks. In some practice settings, doctors or nurses can be designated to carry out certain pharmacy related tasks, so make sure you know who can do what under which circumstances.
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
Board of Pharmacy newsletters are arguably one of the best resources for learning pharmacy law, as they contain interpretations and clarifications issued directed by the Board itself. These newsletters often explain laws, regulations, and rules in greater detail – especially those that are frequently questioned by pharmacists and pharmacy technicians.
For example, the January 2024 Newsletter from the New Jersey Board of Pharmacy specific criteria for evaluating whether to fill a prescription, going well beyond the general guidance of “using professional judgment.” It also provides a more comprehensive explanation of when compounding semaglutide is permissible – offering more clarity than the statute alone. It is very common for MPJE questions to be based directly on content from these newsletters – sometimes verbatim – making them essential study material.
Most states provide links to their newsletters through the NABP website. For example, NJBOP newsletters can be found at https://nabp.pharmacy/bop_members/new-jersey/. Some states may only publish newsletters on their own websites, which can be easily searched and accessed using the internet via search engine of your choice.
The following are some tips you should remember while taking the MPJE:
If state law is silent on a certain issue but federal law covers the topic, then follow the federal law.
If federal law is silent on a certain issue but state law covers the topic, then follow the state law.
If both federal and state law covers the topic, then follow the stricter law.
If both federal and state law are silent on the topic, make an educated guess.
If you do not know the answer to a question, make an educated guess and move on. MPJE is a timed exam, and it is essential to answer all questions before time runs out. Make an educated guess – consider the intent of the question and whether the answer choice you are about to choose is realistic or logic in real world pharmacy practice – and hope for the best. Always keep in mind that your goal is not to get a perfect score but is simply to earn enough points to pass. Interestingly, research from the Center for Teaching at Vanderbilt University suggest that on 5-option multiple choice questions, the answers “None of the above” or “All of the above” are correct 52% of the time – a 90% improvement over random guessing. This is because test writers often use these choices when they want the correct answer to be indisputably accurate or to require qualifying language. So, if you encounter a question where you cannot even formulate an educated guess and one of those choices is available, go for it as we can consider it as an evidence-based guessing.
Oliver Wendell Holmes JR, an associate justice of the SCOTUS, once said “This is a court of law, young man, not a court of justice”. This is the mindset you must adopt to succeed on any law-related exam, including the MPJE. Your focus should always be on identifying the legal issue at hand – not on what may feel morally right or best for the patient.
What is legal is not always what seems ethically ideal. If a question includes extra details that tempt you to make a moral judgment or rely on personal opinion, don’t get distracted. Your job is to isolate and answer the underlying legal question.
It is also important to understand the intent behind laws, rules, and regulations. Consider what regulatory agencies or lawmakers are trying to accomplish. Grasping this intent will not only strengthen your comprehension but will also help you make informed, educated guesses when you are unsure of an answer.
It is common for test takers to feel anxious during the MPJE, especially when faced with a series of challenging questions. Do not panic if this happens to you – it probably is a good sign!
The MPJE is an adaptive exam, meaning the difficulty of questions increases as you answer correctly. If you begin seeing multiple SATA (select all that apply) type questions in a row, take it as a positive indicator. These complex question types are typically only presented when the test algorithm determines you’ve been performing well. In other words, seeing tougher questions means you are likely answering correctly. On the other hand, if you are not encountering many SATA questions or if you are consistently presented with easy questions, take a moment to rest. Breathe, focus, and read each question and answer choices carefully. This is likely why some test takers who describe the exam as difficult end up passing, while those who find it easy may fail.
Watch for keyword such as NOT, MAY, and SHALL – these can significantly change the meaning of a question. Missing them can lead to incorrect answers, even if you understand the topic in depth.
Make sure you understand the definitions of terms as stated in the statutes. For example, many students mistakenly equate the term “age” with “date of birth” while studying for the MPJE, which can cause confusion during the exam when both appear as answer choices.
If a term involves multiple components – such as processes, tasks, or duties – be sure to memorize each part. Take “drug utilization as an example: it includes several specific tasks. Ask yourself, Does it include checking for drug-food interactions?
Also, pay attention to how location-related terms are defined. Unless a question explicitly states the patient is traveling out of state or out of country, the phrase “out of town” means the patient is still traveling within the same state of the MPJE.
Reading definitions carefully and fully understanding what each term means will help you tremendously – especially on SATA questions.
When in doubt during the MPJE, apply common sense and logic.
If you are unsure about an answer, consider the intent and urgency behind the regulation. For example, if a question asks about the deadline for reporting a pharmacist’s change of residential address to the Board, it’s safe to eliminate any answer choices with very short timeframes as it is likely a lower priority for the Board.
In contrast, if the question concerns a pharmacy robbery, eliminate any options with long timeframes. This is a high priority event that the Board would want to know about immediately.
Also, stay mindful of current issues in pharmacy practice. If a question touches on topics like the opioid epidemic, assume the correct answer will likely reflect a stricter regulatory approach aligned with public health concerns.
Take, for example, the New York state law stating: “Unless an earlier refilling is authorized by the prescriber, no prescription shall be refilled earlier than seven days prior to the date previously dispensed supply would exhaust if used in conformity with the directions for use.”
Many interpret this to mean that controlled substances can be refilled seven days early every month – NO! Given New York’s serious opioid crisis, allowing an extra 84 days of opioid supply per year clearly goes against legislative intent. When read carefully, the law actually means that the patient may have at most a 7-day surplus at any one time – not per every fill. This interpretation aligns more logically with the state’s efforts to curb opioid misuse.
No law is written without intent. Try to understand the purpose behind the law, and use context, logic, and current pharmacy issues to guide your answers.
Good Luck!
If you would like to purchase a paper copy of this guide, it is available for purchase at Amazon at MPJE Q-BANK: Study Guide with Questions Only & Interview Tips for Residency Programs: Lee, Alexander: 9798336993202: Amazon.com: Books.
*Disclaimer: This is a personal blog. Any views or opinions represented in this blog are personal and belong solely to the blog owner and do not represent those of people, institutions, or organizations that the owner may or may not be associated within professional or personal capacity unless explicitly stated. All content provided on this blog is for informational purposes only. The owner of this blog makes no representations as to the accuracy or completeness of any information on this site or found by following any link on this site. The owner will not be liable for any errors or omissions in information nor for the availability of information in this blog. The owner will not be liable for any losses, injuries, or damages from the display or use of information in this blog.